Budesonide/formoterol Maintenance And Reliever Therapy In Patients With Difficult-To-Control Asthma
J. Haughney1, R. Buhl2, C. P. van Schayck3, L. Jorgensen4, J. Ostinelli5, M. Aubier6
1University of Aberdeen, Aberdeen, United Kingdom, 2Mainz University Hospital, Mainz, Germany, 3Maastricht University, Maastricht,
Netherlands, 4AstraZeneca Sweden, Sodertalje, Sweden, 5AstraZeneca, Rueil Malmaison, France, 6Hopital Bichat, Paris, France
Corresponding author's email: [email protected]
A31 OPTIMIZING THERAPEUTIC STRATEGIES IN AIRWAYS DISEASE / Thematic Poster Session / Sunday, May 15/8:15 AM-4:30PM / Area C, Hall B (Upper Level), Colorado Convention Center
Introduction
Asthmatic patients who are old, smokers or treated with high-dose inhaled corticosteroids (ICS) are reported to be less responsive to
treatment. Little is known about the effects of budesonide/formoterol (BUD/FORM) maintenance and reliever therapy (Symbicort SMARTR
TurbuhalerR) in these patients. Three pre-planned subanalyses of the EuroSMART study assessed BUD/FORM maintenance and reliever
therapy in these subpopulations.
Methods
EuroSMART (NCT00463866) compared two doses of BUD/FORM, the standard 1x160/4.5ƒÊg inhalation twice daily (1x2) and a 2x160/4.5ƒÊg
inhalations twice daily (2x2) dose, plus as-needed BUD/FORM, in asthma patients (N=8053).1 EuroSMART showed that most patients were
well controlled by 1x2 and that lung function (peak expiratory flow post-bronchodilation <80%) predicted improved responses in favor of
2x2 with regards to exacerbation risk. In this analysis, selected subpopulations were based on age (.65 years vs. 18.64 years), baseline ICS
dose (.1600 ƒÊg/day vs. <1600 ƒÊg/day) and smoking status (smokers vs. non-smokers). Primary endpoint was time to first exacerbation.
Asthma control (ACQ5) and safety (adverse events) were assessed.
Results
Patient demographics are provided in Table 1.
J. Haughney1, R. Buhl2, C. P. van Schayck3, L. Jorgensen4, J. Ostinelli5, M. Aubier6
1University of Aberdeen, Aberdeen, United Kingdom, 2Mainz University Hospital, Mainz, Germany, 3Maastricht University, Maastricht,
Netherlands, 4AstraZeneca Sweden, Sodertalje, Sweden, 5AstraZeneca, Rueil Malmaison, France, 6Hopital Bichat, Paris, France
Corresponding author's email: [email protected]
A31 OPTIMIZING THERAPEUTIC STRATEGIES IN AIRWAYS DISEASE / Thematic Poster Session / Sunday, May 15/8:15 AM-4:30PM / Area C, Hall B (Upper Level), Colorado Convention Center
Introduction
Asthmatic patients who are old, smokers or treated with high-dose inhaled corticosteroids (ICS) are reported to be less responsive to
treatment. Little is known about the effects of budesonide/formoterol (BUD/FORM) maintenance and reliever therapy (Symbicort SMARTR
TurbuhalerR) in these patients. Three pre-planned subanalyses of the EuroSMART study assessed BUD/FORM maintenance and reliever
therapy in these subpopulations.
Methods
EuroSMART (NCT00463866) compared two doses of BUD/FORM, the standard 1x160/4.5ƒÊg inhalation twice daily (1x2) and a 2x160/4.5ƒÊg
inhalations twice daily (2x2) dose, plus as-needed BUD/FORM, in asthma patients (N=8053).1 EuroSMART showed that most patients were
well controlled by 1x2 and that lung function (peak expiratory flow post-bronchodilation <80%) predicted improved responses in favor of
2x2 with regards to exacerbation risk. In this analysis, selected subpopulations were based on age (.65 years vs. 18.64 years), baseline ICS
dose (.1600 ƒÊg/day vs. <1600 ƒÊg/day) and smoking status (smokers vs. non-smokers). Primary endpoint was time to first exacerbation.
Asthma control (ACQ5) and safety (adverse events) were assessed.
Results
Patient demographics are provided in Table 1.
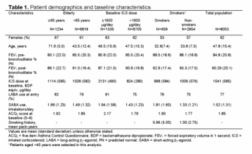
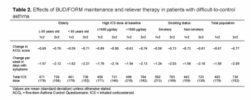
For patients with difficult-to-control asthma (.65 years, .1600 ƒÊg/day ICS at baseline, smokers), there were no significant differences in
time to first exacerbation between the 1x2 and 2x2 treatments. Comparisons between patients with difficult-to-control asthma and their
respective control groups showed that time to first exacerbation was shorter in patients aged .65 years vs. <65 years in both 1x2 and 2x2
groups (P=0.0153 and P=0.0014, respectively) and that, for patients receiving .1600 ƒÊg/day ICS at baseline, there were no significant
differences in time to first exacerbation in the 1x2 or 2x2 groups compared with those receiving <1600 ƒÊg/day ICS at baseline. There was
no significant difference in time to first exacerbation between non-smokers and smokers in the 2x2 group. Overall mean ACQ5 scores and
the number of days per week with symptoms were reduced by both treatments in all patient subgroups. Treatment load (BUD dose,
ƒÊg/day) was similar between subgroups and the total population (Table 2).
Both treatments were well tolerated; the incidence of treatment-related serious adverse events and discontinuations due to adverse
events were similar between treatments in each group.
Conclusions
BUD/FORM maintenance and reliever therapy is an effective asthma treatment concept that also works well in symptomatic patients
considered less responsive to treatment, such as the elderly, smokers or those previously treated with high-dose ICS.
1. Aubier M, et al. Eur Respir J 2010; 36:524–530.
